Normal ingestion of food involves the co-ordinated movements of prehension, mastication and swallowing (deglutition) involving the voluntary prepharyngeal and involuntary pharyngeal and oesophageal phases1. Normal chewing involves proper function of the masticatory muscles and their innervation, temporomandibular joint and oral dental structures. Mild forms of dysmastication or difficulty in chewing may present with a slow masticatory cycle or reduced masticatory force during the normal triphasic chewing cycle (open, close and sliding) or with more severe signs such as quidding / spitting out semi-chewed food, reluctance or inability to move the lower jaw, halitosis and inappetence 1-3. There is considerable overlap with the clinical signs of dysmastication and prepharyngeal dysphagia (difficulty transferring of food from the oral cavity to the pharynx) which include dropping food or water from the mouth, reluctance to chew, ptyalism and abnormalities in prehension. Cases with dysphagia at the level of the pharyngeal and oesophageal anatomical regions typically present with an extended neck position, pain or swelling in the throatlatch region, anorexia, inappetence, nasal discharge containing saliva, water or food material or a cough associated with aspiration pneumonia1,2.
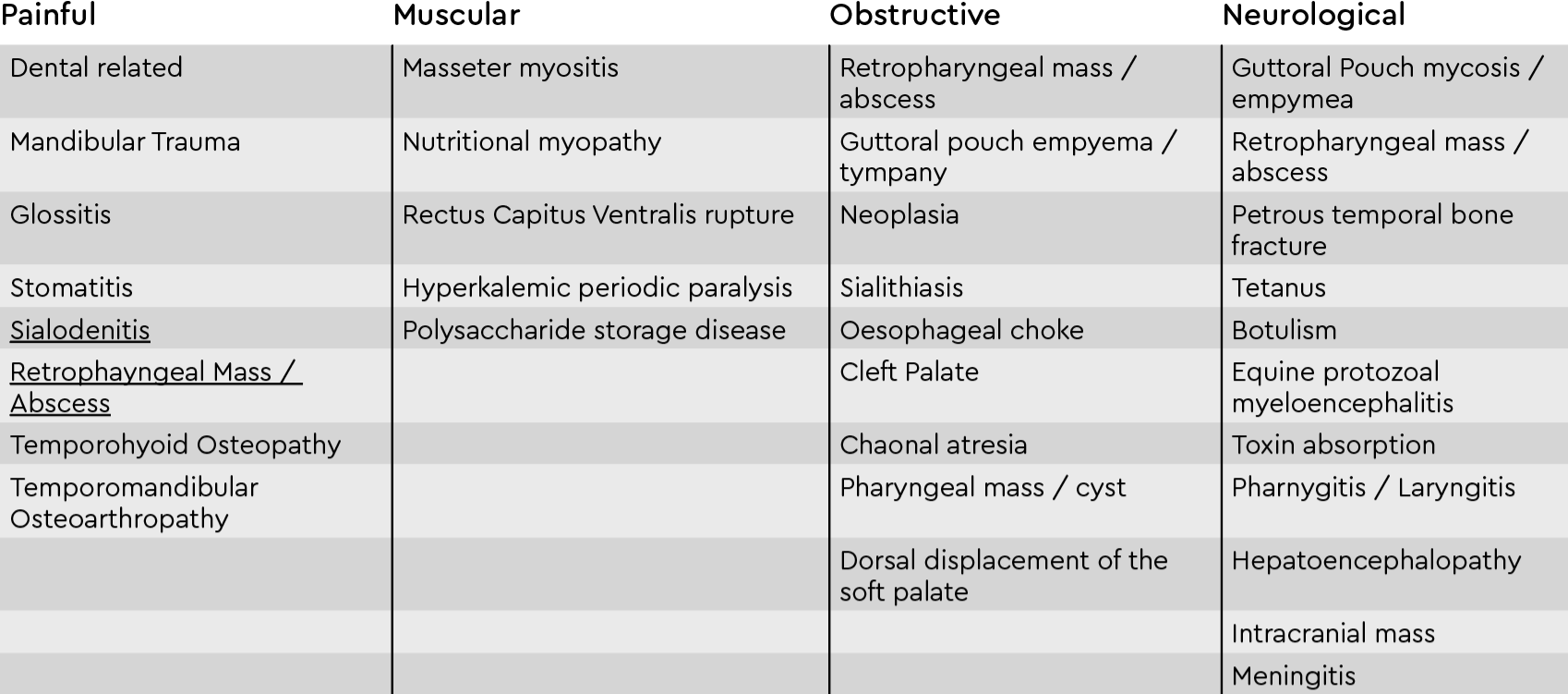
Dysmastication and dysphagia can be divided into four types: painful, muscular, neurological and obstructive. Painful and obstructive causes interfere with the mechanism of prehension, bolus formation and transfer to the pharynx region4-12. Muscular and neurological causes impede prehension by affecting the motor function of the lingual and buccal musculature, restricted or impaired movement of the muscles of mastication, with restricted ability to open the mouth (trismus) 13-14. Sensory loss to the lips, buccal mucous membranes, tongue, pharynx or larynx can cause dysphagia. Neurological causes may arise from the forebrain, brainstem or peripheral nerves that control prehension (Vm, Vs, VII, XII), transfer of food bolus to the pharynx (Vs and XII) and swallowing (IX and X)1, 2, 15.
Specific questions relating to vaccination history, diet, involvement of other systems such as respiratory signs (nasal discharge, coughing) and progression of the presenting signs (weight loss and degree of quidding or inappetence and behaviour changes) are important details to help identify the cause of dysmastication.
A general clinical and neurological examination including cranial nerve functions will help determine if there is evidence of a systemic disease distant to the oral cavity. External palpation of the salivary glands, the masticatory muscles, cheek folds, bony contour of the skull region, in particular the temporomandibular joints, the base of the ears and regional lymph nodes can identify focal areas of swelling, crepitus or fistulous tracts which may induce a painful evasive response. Initial assessment of the oral cavity including visual assessment of the incisor mucogingival health, the incisor bite plane and the ability to open the mouth and move the mandible and assess the position and mobility of the tongue are important steps before sedating the patient and placing a mouth speculum.
Further assessment of the skull, oral cavity, pharynx and larynx can be performed using imaging modalities; oroscopy, rhinoscopy, ultrasonography, radiography, computed tomography, magnetic resonance imaging and histology of biopsies. Secondary dental changes such as increases in obliquity to the occlusal plane of the incisors (slant mouth) and cheek teeth (shear mouth) may occur due to a chronic painful or restricted masticatory cycle.
Differential Diagnosis for Dysmastication & Dysphagia in the Horse:
1 Reed, Stephen M; Bayly, Warwick M; Sellon, Debra C. Equine Internal Medicine, Fourth edition (2018); 268-272,584, 792-796.
2 Easley, Jack; Dixon, Padraic M; Du Toit, Nicole Equine dentistry and maxillofacial surgery (2022); 99-110, 207-272, 287-301
3 Reardon, R. (2018) Managing Dysmastication in Horses: An Update. In Practice 40:3;115-121.
4 Kilcoyne I, Watson JL, Spier SJ, Whitcomb MB, Vaughan B. (2015) Septic sialoadenitis in equids: a retrospective study of 18 cases (1998-2010). Equine Vet J. 47(1):54-9.
5 Carlson N, Eastman T, Winfield L. (2015) Sialolithiasis in horses: A retrospective study of 25 cases (2002-2013). Can Vet J. 56(12):1239-44.
6 Pelzel-McCluskey, A.M. Vesicular Stomatitis Virus. Veterinary Clinics North America: Equine Practice 39 (2023): 147-155.
7 Pusterla N, Latson KM, Wilson WD, Whitcomb MB. (2006) Metallic foreign bodies in the tongues of 16 horses. Vet Rec. 159(15):485-8.
8 Carmalt, J.L. (2014), Equine TMJ disease. Equine Veterinary Education, 26: 64-65.
9 Smyth, T., Allen, A.L. and Carmalt, J.L. (2017), Clinically significant, nontraumatic, degenerative joint disease of the temporomandibular joints in a horse. Equine Vet Educ, 29: 72-77.
10 Magri, C., Schramme, M., Nottrott, K., Schweizer-Gorgas, D., Segard, E., Kelly, G. and Schumacher, J. (2021), Coronoidectomy as a treatment for mandibular immobility caused by fracture of the coronoid process in three horses. Equine Vet Educ, 33: e331-e337.
11 Tanner J, Spriet M, Espinosa-Mur P, Estell KE, Aleman M. (2019) The prevalence of temporal bone fractures is high in horses with severe temporohyoid osteoarthropathy. Vet Radiol Ultrasound;60(2):159-166.
12 Hall NP, Ragle CA, Farnsworth KD, Caffey SR, Sanclemente JL. (2021) Treatment of temporohyoid osteoarthropathy in horses with a basihyoid-ceratohyoid disarticulation technique: 6 cases (2018-2019). J Am Vet Med Assoc. 259(3):300-305.
13 Aleman, M. (2023) Brief review of masseter muscle disorders. Equine Veterinary Education, 35, 305–310.
14 Wilson, A., Talbot, A., Crosby-Durrani, H. & Malalana, F. (2023) Masseter myodegeneration in the horse: Suggested approach to diagnosis and treatment. Equine Veterinary Education, 35, 300–304.
15 Swink, J.M., Gilsenan, W.F. (2022) Clostridial diseases (Botulism and Tetanus). Veterinary Clinics North America: Equine Practice 38: 269-282.
